
Physical activity: an answer looking for a question.
The reasons why physical activity is good for us have changed over time. The history of these changes may surprise you.

I was recently invited to present at the Western Sydney Moving community of practise (https://www.wsydmoving.com.au). This group meet monthly and are, generally, made up of people who believe that physical activity is good for us. They are academics, health professionals, exercise physiologists and strategy makers trying, in their own way, to improve population health by advocating for physical activity. A laudable cause.
I have sat in other sessions in which presentations have been given by those more learned than me and observed the collective head nods and gesticulations from audience members signalling their approval of the messages conveyed. They were, at least in my view, preaching to converted, something I have become more and more aware of in recent years, at conferences we attend, not to learn or be challenged, but to have our preconceptions and biases confirmed.
It was for this reason I wanted to present a series of counter points to the movement toward physical activity as a universal good and highlight areas where the consensus doesn’t seem, at least in my opinion, to align with practise or, dare I say, the view of the common person in the street. This is not to say I don’t believe nor value the impact that physical activity has on health, I do. The message, however, too often gets hijacked by the modern disease of overstating benefits and extrapolating data to such an extent that the claims made become quite unbelievable. I’ll try and substantiate this comment when I discuss the trend for reporting the financial impact and benefit of more people being physically active.
The presentation lasted 25 minutes and consisted of 26 slides, most of which were filled with photos so to guide my thought process. I tried to focus on the landscape in the United Kingdom, largely because I have more experience of that system and also because it is often easier to be objective around the decisions others make than those we have made ourselves.
Over the next couple of weeks, I’ll try to put some meat on the bones and articulate in greater depth the key themes of the session. Within the Substack articles ill post some of the slides and publish the presentation in full for anyone interested.
A changing rationale
The case for physical activity is, as I see it, two pronged. Firstly, there is the need to convince those who hold the purse strings that funding initiatives and organisations that support growth (or at least attenuate the decline) in physical activity is money well spent. Secondly, there is a need to appeal to the hearts and minds of the general population, so they understand, are empowered, and supported to be physically active. The arguments made by those advocating for physical activity have changed over time. Initially they focused on the need to improve health in the name of national security. The country would not be able to wage war if those recruited to bear arms were of poor health and physical fitness, something which was on the mind of those in power at the time of the Boer wars. The rationale shifted in the 1990’s, focusing on better health to reduce costs associated with treating lifestyle related disease and the financial burden on the welfare state. This has, in the 2000’s, morphed into using physical activity as a lever by which the benefits of sport can be realised, as a toll to advocate for inclusivity and tackle loneliness and isolation. One might be forgiven for thinking it warranted the title of panacea.
The historical perspective
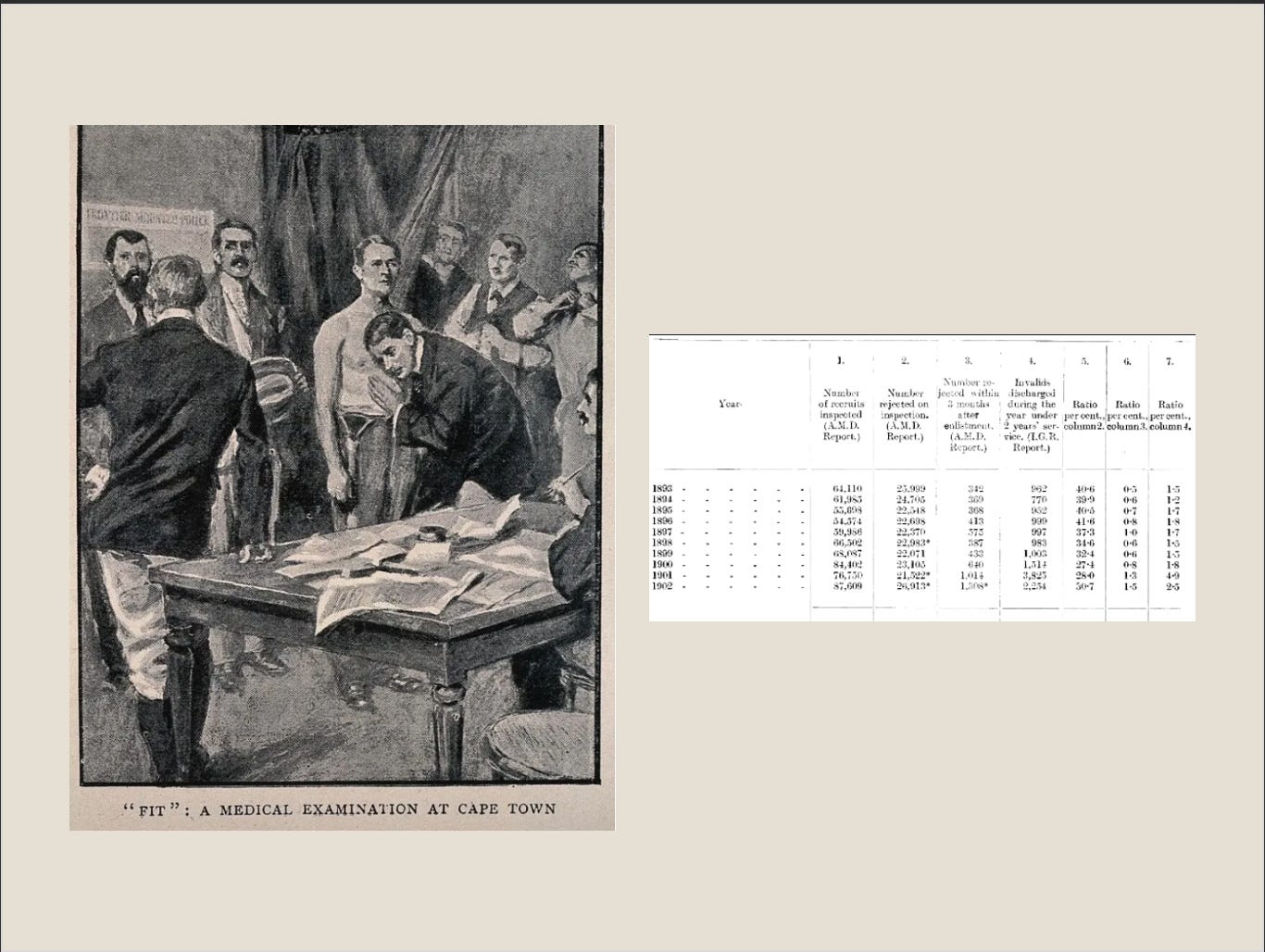
In the early 1990s the case for increasing physical activity levels among the working classes in the United Kingdom was in response to the physical condition of recruits to the armed forces. The argument focused on the need for changes at the societal level that would improve the physical condition of men required to take up arms and defend their country in future wars. The Fitzroy report, authored in 1904, detailed the physical condition of army recruits, you can find the full report here and a quote from the report is detailed below:
“it is a most disturbing fact that from 40 to 60 per cent of the men who present themselves for enlistment are found to be physically unfit for military service.”
The authors, with an alarming degree of prescience, highlighted the futility of explaining physical activity levels, something modern-day research is still intent on doing. Rather, the authors recognised that once the problem had been identified, continuing to describe it was futile. Instead, efforts should be redirected to address the issue. I wonder, how much progress we have made in the intervening 122 years when it comes to advancing health through physical activity among the proletariat?
Worth noting is that the focus of the Fitzroy report was the working man or, what in today’s parlance would be described as hard-to-reach groups (encompassing men and women from lower socio-economic backgrounds and living in some of the poorest areas), especially when discussing adherence to being physically activity. In 1904 this represented the parts of society recruited to fight for their country and who would, in peace time, be tasked with some of the hardest jobs, in the toughest conditions, and with the least amount of pay. For anyone who has read The road to Wigan Pier by George Orwell published some 32 years after the Fitzroy report, it is hard to imagine those who spent their working day hunched over underground would want, at the end of their shift, to engage in physical activity. Even Zumba has a limit to its appeal!
Although the rationale for increasing physical activity levels in this group has changed over time, we are still unable to reach and support those groups who could benefit the most from increasing their physical activity. Poverty, ill health, and a lack of opportunities to be physically active are as intrinsically linked now as they were in 1904.
Time is a great healer
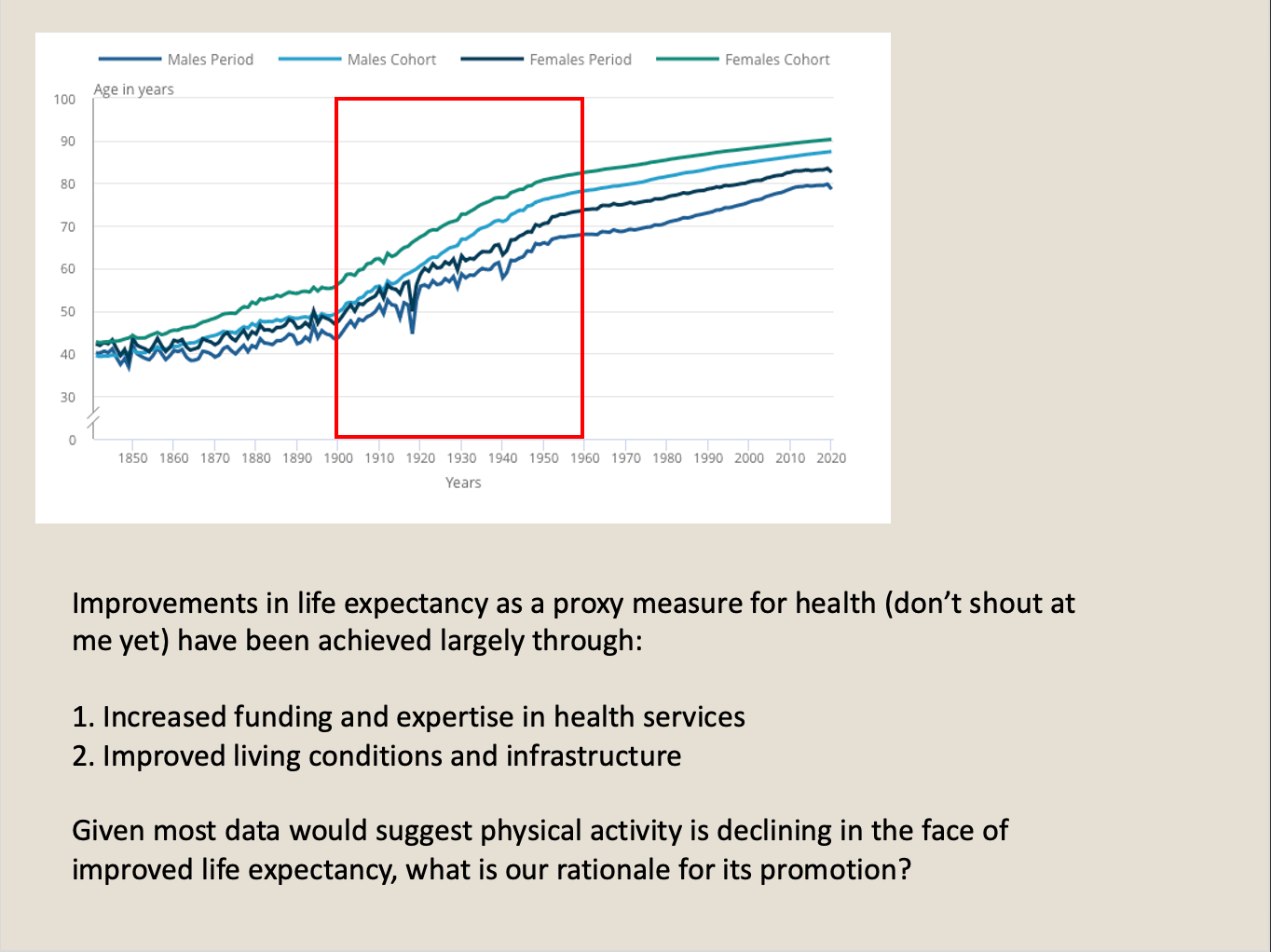
A lot has changed since 1904 and population health data would suggest that life expectancy has increased exponentially. Good news indeed. These changes, however, have largely been brought about by improvements in infrastructure during the 1940s and 50s as well as, in more recent times, the steady march of technology and cannot be attributed to changes in physical activity. Let me explain.
If we look at data on life expectancy in the United Kingdom as an example (you can review the statistics here and the corresponding slide is pictured below) we see that the trend towards people living longer started in the late 1800s and accelerated in the mid 1900s. Why? In the late 1800s many of the main cities in England started to develop large swathes of green space for the enjoyment of those who lived in the area. They were, unlike the Roman Baths of Esquiline Hill, egalitarian and designed to benefit everyone in society from the richest to the poorest. The ribbon of parks in Liverpool (UK), my home city, is one such example. Sefton Park was bought in 1867 for $250,000 from the Earl of Sefton and continues to this day to provide opportunities for the local community to be active in and around green and blue space. Access to such amenity was a factor in at least some of the improvements in life expectancy through the end of the century as well as the mechanisation of many of the most labour-intensive jobs in industrial Britain.
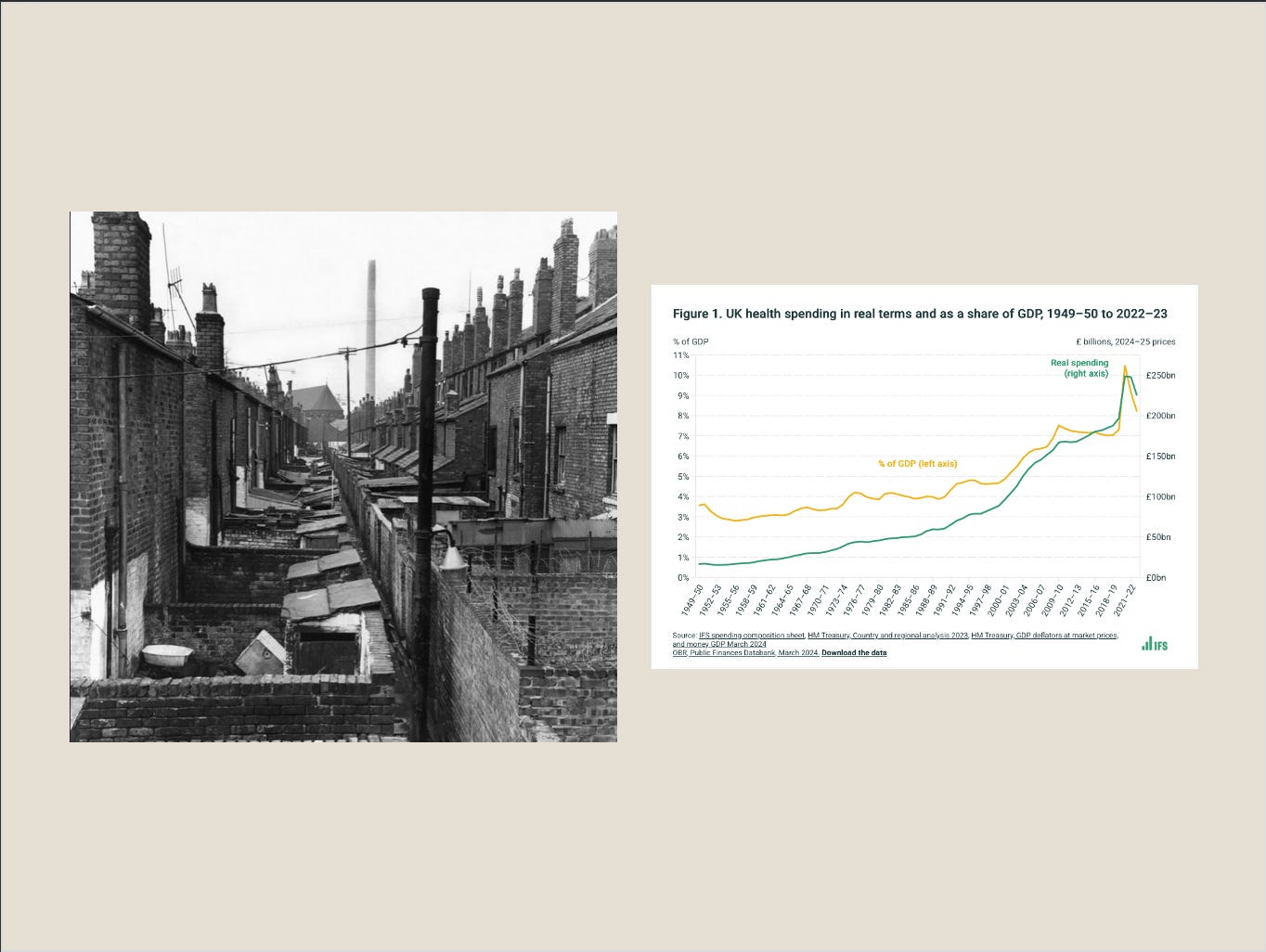
Another big change came in 1940s. After the second world war the UK embarked on its welfare state, including the National Health Service and increased funding focused on better health outcomes for the population. This investment was coupled with reforms that allowed cities and councils to improve their housing stock, improve sanitation, clear slums, and create new towns for a growing populace. Infrastructure, both improved housing and accessible green space, coupled with a welfare state, have, it would seem, done the most to improve life expectancy, at least in the UK. Physical activity has had a bit part role at best which challenges the long-held notion that it is a key component in maintaining and improving public health.
The march of technology
In the same way improvements in infrastructure advanced life expectancy in the late 1800s and mid 1900s, it is technology that has taken over in the 2000s, delivering greater benefit to health outcomes that physical activity may ever hope to achieve.
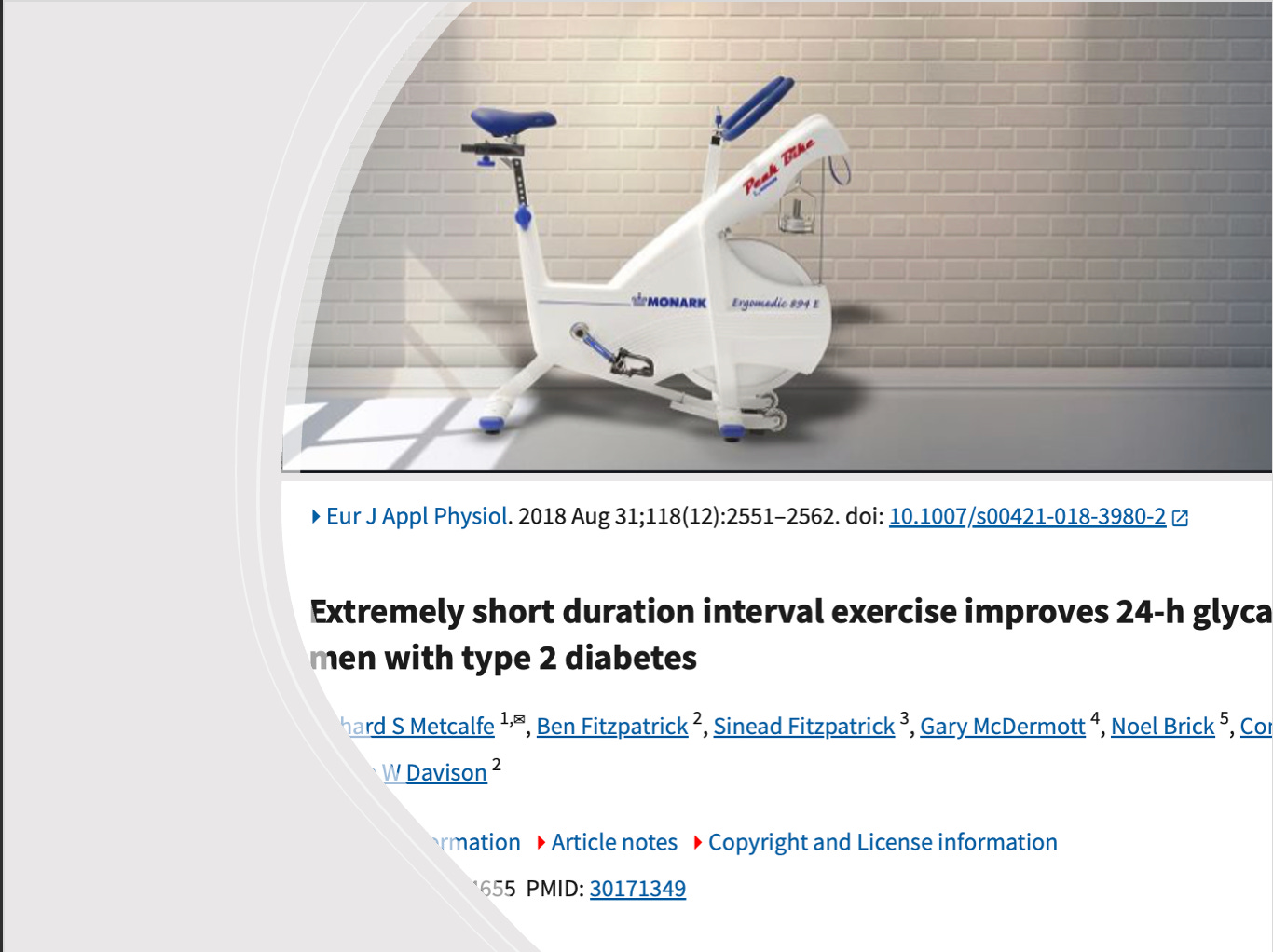
Back in 2018 I was aware of research being conducted on a university campus in Edinburgh which aimed to improve glycaemic control in Diabetes patients using high intensity exercise. The methodology required patients to perform supramaximal exercise, that is, all-out efforts on a cycle ergometer. The efforts ranged from 20-30s across a series of up to four repetitions. The protocol was more akin to what you might see an athlete attempt when trying to improve their repeated sprint ability rather than a patient in a clinical setting. The results, however, were surprising, at least to me.
The exercise worked. Those who participated in the experiments improved glycaemic control. Patients struggling to control their diabetic symptoms and who were often overweight could fight back with an exercise regime that took no more than 5 minutes to complete. Who doesn’t have 5 minutes to partake in something medically proven to improve health? Well, quite a few people, it would seem.
The problem with supramaximal exercise is that it is hard and not very enjoyable, especially if you are not accustomed to exercise. Statistically speaking, most people suffering from issues relating to diabetes or obesity are unlikely to regularly engage in exercise and physical activity. Perhaps this is a methodological issue with much of the research? Those who design exercise interventions are already convinced of their benefit and are likely active themselves. It is hard to understand why people do not engage with something you enjoy when you are convinced of the benefits it has. How often have you heard someone with access to green space and the time to for physically active leisure pursuits lament that those with poor health because of inactivity should just ‘exercise more’. Researchers are not immune from this cognitive bias. The result? Uptake was low and the rise in obesity, diabetes and other lifestyle related illnesses continues to increase. You can view changes in the prevalence of obesity and how it is concentrated in the poorest parts of the country here https://ukhsa.blog.gov.uk/2021/03/04/patterns-and-trends-in-excess-weight-among-adults-in-england/).
In the intervening years technology is solving a problem that physical activity could not. The rise in GL-1 drugs (you may be more familiar with the brand name of Ozempic) are revolutionising diabetes care and how patients are supported to lose weight. Such is their effectiveness they are now as much a lifestyle drug as a clinical intervention, even if that was not the original intention. In a separate field, E-bikes are changing the face of active travel and doing more to promote cycling than even the most well-intentioned cycleway infrastructure could have ever hoped to achieve. Technology continues to lead the charge toward healthier lifestyles.
This leaves physical activity in a tricky spot. For many years its reason for being was an antidote to poor health, to reduce the symptoms of lifestyle related disease and help governments reduce the cost of public health. The data would suggest that, when compared to other approaches to the problem, it has been spectacularly ineffective. It is perhaps for these reasons that physical activity in the 2000s has begun to look for other questions for which it may be an answer. We will deal with those in next week’s post.